Your first seven vertebrae (C1 – C7) are located within your neck and are known as your cervical vertebrae. The cervical vertebrae are supported and cushioned by intervertebral discs. Damage to a disc, either due to injury or disease, can lead to debilitating nerve pain, nerve damage, and loss of mobility. In severe cases, cervical artificial disc replacement may be your best solution.
What is cervical artificial disc replacement?
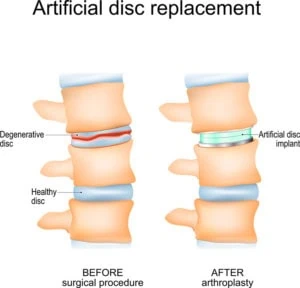
Artificial disc replacement (ADR) is a surgical procedure in which a damaged disc is replaced with a new, synthetic disc. ADR is sometimes referred to as total disc arthroplasty or total disc replacement, so don’t be alarmed if you hear the terms used interchangeably. Cervical artificial disc replacement is a type of ADR surgery specifically performed on the discs between the cervical vertebrae (as opposed to the thoracic or lumbar vertebrae).
Cervical artificial disc replacement surgery is performed under general anesthesia. The surgery typically lasts one to two hours. During the surgery, a one to two inch incision is made near the front of the neck. Soft tissues (the skin, fat, muscle, and trachea) are pulled to the side in order to expose the cervical vertebrae underneath. The damaged disc is then removed, and the artificial disc is inserted into place. There are currently five different artificial discs approved by the FDA for use in cervical ADR.
Is cervical ADR effective?
You can trace the history of cervical ADR all the way back to the 1960’s. The evidence amassed over time has proven again and again that cervical ADR is not only effective but also superior to the more traditional surgery, spinal fusion. Cervical ADR successfully relieves nerve pain and nerve damage caused by the following:
Degenerative disc disease
As you age, the discs between your vertebrae begin to dry out and flatten. The natural deterioration of your discs is called degenerative disc disease. Degenerative disc disease can lead to problems such as bone spurs, cervical stenosis, cervical radiculopathy, herniated disc, and cervical myelopathy.
Cervical radiculopathy
Cervical radiculopathy is a condition in which a damaged disc pushes upon a nearby nerve. It’s colloquially known as a “pinched nerve.” Cervical radiculopathy can be felt as pain, tingling, or weakness extending from the shoulders or down the arms.
Herniated disc
A herniated disc is a disc that has ruptured in such a way that some of the inner portion of the disc has bulged out into the spinal canal.
Cervical myelopathy
Cervical myelopathy is a condition in which the spinal cord is compressed by a herniated disc or bony growth. This can result in neck pain, neck stiffness, reduced fine motor skills, and balance problems.
What are the potential benefits of cervical ADR?
Cervical ADR has the potential benefits of:
- Correcting disc degeneration in one to two discs
- Relieving pain caused by nerve compression
- Restoring normal neck motion and flexibility
Should you choose cervical ADR or fusion?
Despite the rising popularity of cervical ADR, another procedure is still considered the more time-worn and traditional approach. This procedure is known as anterior cervical discectomy and fusion (ACDF). Anterior cervical discectomy is a fancy way of saying a cervical disc is removed from the anterior, or front, of the neck. The fusion part of the surgery occurs after the cervical disc is removed. The cervical vertebrae are then fused together via a bone graft, metal plate, and screws. There is no artificial disc implanted during ACDF.
With the availability of two procedures, a question arises. Is artificial disc replacement better than fusion? In summary, cervical ADR has several advantages over ACDF. These advantages are explained below:
- Cervical ADR preserves your natural neck motion and flexibility. ACDF will limit your range of motion and flexibility.
- Cervical artificial disc replacement recovery is less intensive than that for ACDF. Recovery time for cervical ADR is 4 to 6 weeks with no need to wear a cumbersome neck brace. On the other hand, ACDF requires a neck brace to be worn for weeks after surgery. It’s a long 12 to 18 months before the vertebrae are considered completely fused together.
- With ACDF, the vertebrae above and below the fused segment experience higher biomechanical stress. This can lead to increased degeneration of the cervical discs above and below the fused segment. In some cases, additional surgery is needed after ACDF to correct the degeneration of an adjacent segment. On the other hand, cervical ADR poses a low risk for adjacent segment degeneration.
Know that there are some situations in which ACDF is a better choice (i.e., if you have osteoporosis or ankylosing spondylitis). Trust that your doctor will tell you what surgical approach is best for you.
Is surgery the best option?
One should only resort to surgery after all minimally-invasive and/or non-surgical techniques have been attempted. Non-surgical techniques include rest, heat, ice, pain medication, physical therapy, and chiropractic care. Surgery is only considered after these techniques have failed, and symptoms have persisted for at least four to six weeks.
How do you know if you’re a good candidate?
Who is a candidate for artificial disc replacement? Overall, candidates for cervical ADR must be healthy individuals that are at least 18 years old and possess skeletal maturity. The patients of cervical ADR typically range from 20 to 70 years of age.
Only your doctor can determine if you are a good candidate for cervical ADR. Their decision is based on your overall health and diagnostic testing (i.e., X-rays, MRI, and CT scan). There are contraindications that will prevent cervical ADR. These contraindications include, but are not limited to, the following:
Advanced spinal degeneration
Advanced spinal degeneration presents many problems that cannot be fixed by cervical ADR. For example, an ossified longitudinal ligament or degraded facet joint cannot be corrected by cervical ADR. In addition, cervical ADR cannot be performed when 3 or more adjacent cervical discs need to be replaced.
Weak bones
Osteoporosis or bone infection can lead to weakened bones. If the bones are too weak, the artificial disc is less likely to remain in place.
Allergy
Cervical ADR is not possible if you have an allergy to any of the artificial disc materials. The materials can include polyethylene, stainless steel, titanium, and cobalt-chrome.
How do you prepare for cervical disc replacement surgery?
There are activities that can help you prepare for an upcoming cervical ADR. These activities can be done in the weeks before surgery and are discussed throughout our Total Disc Arthroplasty & Total Disc Replacement page. Activities include reviewing all medications, undergoing tests and blood work, adhering to self-care instructions (i.e., stop smoking), and developing a support system of friends and family.
Potential complications with the procedure
There are potential risks and complications for any surgery. Fortunately, the rate of complications for artificial cervical disc surgery is low. Potential complications associated with cervical ADR include:
- Nerve or spinal cord injury
- Excessive bleeding
- Excessive pain
- Infection at the surgical site
- Reaction to the foreign material
It’s important that you discuss the potential risks and complications with your doctor before having cervical ADR. Your doctor will help you weigh these potential complications with the benefits of having the surgery.
What is the recovery process after ADR?
Your time at the surgery center or hospital may last anywhere from four to 24 hours, depending on whether the cervical ADR is an outpatient or inpatient procedure. Upon waking from the procedure, you may experience temporary neck and/or arm pain, difficulty swallowing, or voice hoarseness. Prescription pain medication is offered for the first week after surgery.
Everyone heals at different rates, so it is hard to pin-point an exact time frame for your own recovery. Some individuals can return to light work after just one week. In general, patients return to their normal routines within four to six weeks. Physical therapy is initiated around four weeks after surgery.
Choosing your surgeon
Electing to have cervical ADR is a big decision to make. Another big decision to make is deciding on who will be your surgeon. You should choose a spine surgeon who has extensive experience in cervical ADR. Be comfortable with asking questions. One question to ask is, “How many cervical disc replacements have you performed?” Another question to ask is, “How does your complication rate compare to the national average?”
The doctors at The Spine Center are dedicated to answering all the questions you may have. They have over 50 years of experience with treating spinal conditions and are determined to offer you the care that you need. Feel free to contact The Spine Center and schedule a consultation. Contacting The Spine Center will only get you closer to a life without pain.